Downtown Eastside academics at the BCCSU work alongside first responders to reduce B.C. overdose deaths
Vancouver paramedics and firefighters receive a lot of credit for the extra burden they’ve carried since fentanyl arrived in B.C. and sent overdose calls skyrocketing. The same goes for social-service providers and staff at supervised-injection sites. To be sure, they all deserve praise. But there’s another group working to prevent deaths—one that’s a step removed from the frontlines—that receives less attention.
In a supportive role are research organizations that inform on-the-ground efforts and help government officials improve services for overdose prevention and response.
They include the B.C. Centre for Excellence in HIV/AIDS, the B.C. Centre for Disease Control, universities (including UBC and SFU), and, located in Vancouver’s Downtown Eastside—the epicentre of the crisis—there is the B.C. Centre on Substance Use (BCCSU).
Ryan McNeil is a research scientist and team leader with the BCCSU. He told the Georgia Straight they’ve worked with a half-dozen of Vancouver’s new overdose-prevention sites since the provincial government began funding them in late 2016.
“We can feed findings and recommendations back to the groups operating these services and also to the people making decisions about them,” McNeil said in a telephone interview. “In practice, this has meant our on-the-ground social-science work has an impact in informing the overdose response.
He provided an example: since December 2016, the BCCSU has followed about 70 people who regularly use an injection site in the Downtown Eastside. After a few months, a common sentiment emerged from some of this group’s female members. They didn’t always feel comfortable accessing harm-reduction services in locations where male clients were present, McNeil recounted. In response, the BCCSU entered into discussions with the nonprofit Atira Woman’s Resource Society, which had just begun operating a small women-only injection site. The BCCSU shared its data with Atira leadership, who then drew on that data to inform best practices at what became Sister Space: North America’s first and only women-only supervised-injection facility.
Later, the Northampton, England–based Society for the Study of Addiction published an academic paper: “Participants indicated that OPS were…gendered and racialized spaces that jeopardized some women’s access,” it reads. “Although women who use drugs in Vancouver, Canada appear to feel that overdose prevention sites address forms of everyday violence…these sites remain ‘masculine spaces’ that can jeopardize women’s access.”

In another example, McNeil and his BCCSU colleagues evaluated grassroots efforts inside privately owned single-room occupancy (SRO) hotels wherein activists distributed the opioid-reversal drug naloxone and taught tenants how to respond to an overdose. “Opportunities and Challenges from a Tenant-Led Overdose Response Intervention in Single Room Occupancy Hotels,” reads the title of the article that was eventually published in the Journal of Urban Health.
Next, BCCSU staff and members of the Tenant Overdose Response Organization—the BCCSU’s partner on the project—met with City of Vancouver officials and convinced them to establish similar programs in additional SROs.
“[The trial program] was highly successful in expanding naloxone availability and ensuring that people were trained and able to administer it,” McNeil said. “That, in turn, directly informed the decision to scale up that program across a wider set of hotels in the neighbourhood.”
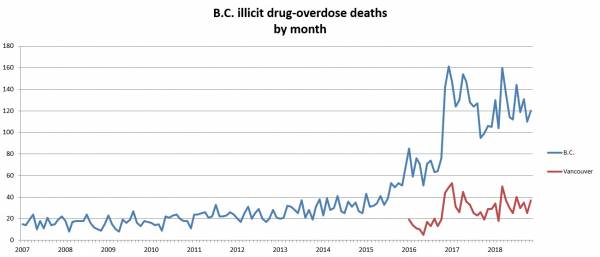
There were an estimated 1,500 illicit-drug overdose deaths in B.C. last year, up slightly from 2017, when there were 1,486, and miles above the 333 deaths that were recorded five years earlier, in 2013.
In a telephone interview, BCCSU director Evan Wood noted the extent to which B.C. health authorities are still catching up to the scale of this crisis. “For people with addiction, we need to treat this as a disease,” he told the Straight. “Up until very recently, we didn’t even have guidelines for the treatment of opioid addiction.” (It was the BCCSU that finally did publish opioid-addiction treatment guidelines for B.C., in June 2017.)
In addition to research, Wood described a second role that the BCCSU plays behind the scenes in the province’s response to the overdose epidemic. The organization is helping hospitals build and integrate models for addictions care, he said, and is providing training in order to equip hospitals to staff those systems.
Woods explained with an analogy: “If you go into any emergency room in British Columbia with chest pain, you’ll get on the chest-pain pathway,” he began. “If you’re having a heart attack, you’ll get medications to address an acute coronary syndrome. Then, once the acute incident is over, before you leave the hospital, you’ll get medications to prevent a heart attack from happening again. You’ll get a follow-up appointment with a specialist, you’ll get a letter dictated to your family doctor, and an expectation that you see your family doctor within a week. You’ll get counselling around diet and exercise and smoking cessation, if that’s relevant. A whole chronic-disease model gets applied.”
When someone is admitted to a hospital for a drug overdose, Wood continued, there is generally no system in place to send that individual down a comparable “addiction-care pathway”. (He noted there are exceptions, such as St. Paul’s Hospital in Vancouver.)
“The emergency-room physicians will do a great job giving you Narcan [the overdose-reversal drug also known as naloxone] and resuscitating you, but none of that addiction-care pathway would be offered,” Wood said. That’s something the BCCSU is working with B.C.’s regional health authorities to change, he added.
Wood said the BCCSU has also helped streamline certain areas of training for the managing of addictions: for example, the process by which a B.C. doctor is licensed to provide opioid-agonist therapy (OAT).
OAT, or medication-assisted treatment (MAT), as it’s known in the United States, includes the use of prescription drugs such as methadone, Suboxone, and, in some cases where those traditional treatments fail, injection-hydromorphone or diacetylmorphine. These medications help an individual addicted to opioids to manage their cravings. In the past, if a doctor in B.C. wanted to offer these treatments for addiction—treatments with significantly higher success rates than abstinence-based methods, studies show—they had to pay a fee and attend a course that was only offered once a year. That meant there were only a small number of doctors in B.C. properly trained to treat a drug addiction, Wood said.
“Now we’ve made it so that 365 days a year, you can do the course online,” he continued. “And it’s free. And then you can do the in-person practicum component in your home community.”
Wood said the province is catching up and improving addictions care but that there’s still a long way to go. “It’s an area that has been neglected for so long,” he explained.













Comments